| Click here to take the CNE quiz for our CNE-eligible article, "Disaster Preparedness at Health Centers" from the Spring 2026 issue of Streamline. Available from June 5, 2026 through December 1, 2026. |
In the summer of 2024, Hurricane Beryl tumbled into Texas, breaking many records as it reached landfall, including earliest Category 5 hurricane in the Atlantic basin; strongest maximum sustained winds for an Atlantic hurricane before August; and fastest intensification in 24 hours for an early storm. A month before Beryl, Houston had experienced a powerful derecho windstorm that blew out windows in high-rise buildings and caused extensive damage to electrical infrastructure. Hot on Beryl’s heels was a heat wave that brought record-breaking temperatures for many days across the entire American West. Due to an aging electrical grid unprepared for high winds and still reeling from the derecho, Beryl knocked power out for over 2.6 million people, who struggled to stay cool in the heat that followed. These three back-to-back weather disasters turned infrastructure weaknesses into health crises. In Houston in the aftermath of Beryl, the state set up an emergency field hospital in a sports arena to support overwhelmed hospitals. However, with the extended loss of power, patients who had stabilized could not be discharged, due to the absence of safe, temperature-controlled discharge locations. Cell service was out, leaving people unable to make emergency calls. Downed power lines and trees, flooding, and other debris and road damage slowed ability to access care. Within such an atmosphere, health center patients struggled to manage their chronic illnesses, cool their medicines, access appropriate foods, and access health care if illnesses became exacerbated.
Most communities are vulnerable to at least one extreme weather event such as prolonged heat, flooding, drought, hurricanes and other severe storms, extended periods of poor air quality, heavy snowfall, or tornadoes and other high-wind events. Many communities face risks from more than one of these hazards, sometimes within the same calendar year, as Houston experienced.
Clinicians at community health centers have a unique and important role in anticipating the types of weather hazards that could occur in their community. Preparations for such events are not limited to the narrow needs related to the weather itself, but must consider a much wider range of infrastructure instabilities, policy consequences, historical pressures, and current events that may compound the consequences of a weather event and its aftermath. Health centers must consider how the weather event, and the aftermath of the weather event, might affect:
- Ability to adhere to laws and regulations, like health and safety regulations at work,
- Ability to carry out emergency management plans,
- Access to care by all members of the community, and
- Long-term endurance of infrastructure.
Additionally, health centers must consider overlaps between crises. In the case of Houston, the derecho, hurricane, and heat wave occurred when electrical infrastructure was already weakened and aging. In California, the deadliness and danger of the Los Angeles wildfires of 2025 were compounded by the high population density in the burn area, the failure of emergency alert policies that were outdated and not functioning properly, and staffing shortages among emergency responders.
The health outcomes of these compounding factors – weather emergencies, sometimes more than one at one time, overlayed on policies, systems, and regulations that may help or complicate emergency response and recovery – are wide. Displacement, impact on mental health, illnesses and injuries, both new and exacerbated, and deaths must each be considered in an emergency plan.

Displacement & Movement
People who are displaced or moving relating to an extreme weather event can be placed into three categories. A clinic’s approach to each category may differ. People may fall into more than one of these categories, as well.
1) Weather-Precipitated Individuals are people who move because of a disaster and/or its aftermath. When such individuals stay within national borders, they are termed “internally displaced people” or IDPs. The timeframe for displacement among weather-precipitated individuals varies greatly. This may range from a household that is evacuated before a hurricane for just a few days, to a family whose house has burned down in a wildfire, not returning for several years, to a community experiencing ongoing flooding in which many families choose never to return. Many who depart their homes in an emergency arrive in a new service area without records of their health needs or ongoing treatments, and often live in temporary accommodations like hotels, the homes of friends or relatives, or evacuation centers. Those who need to stay away from their homes for longer periods of time may need to move several times before they are settled.
2) Weather-Impacted Individuals are people who choose to move – for a new job, for more opportunity, to reduce their cost of living – but experience hardship and challenges related to a weather event during or after their move. For example, a farmworker family relocated to a new agricultural region for work. Soon after moving, the region experienced unprecedented flooding. The family was not well integrated into community and was unaware of resources that may be available to help in emergencies or to assist the family with evacuation options available to them.
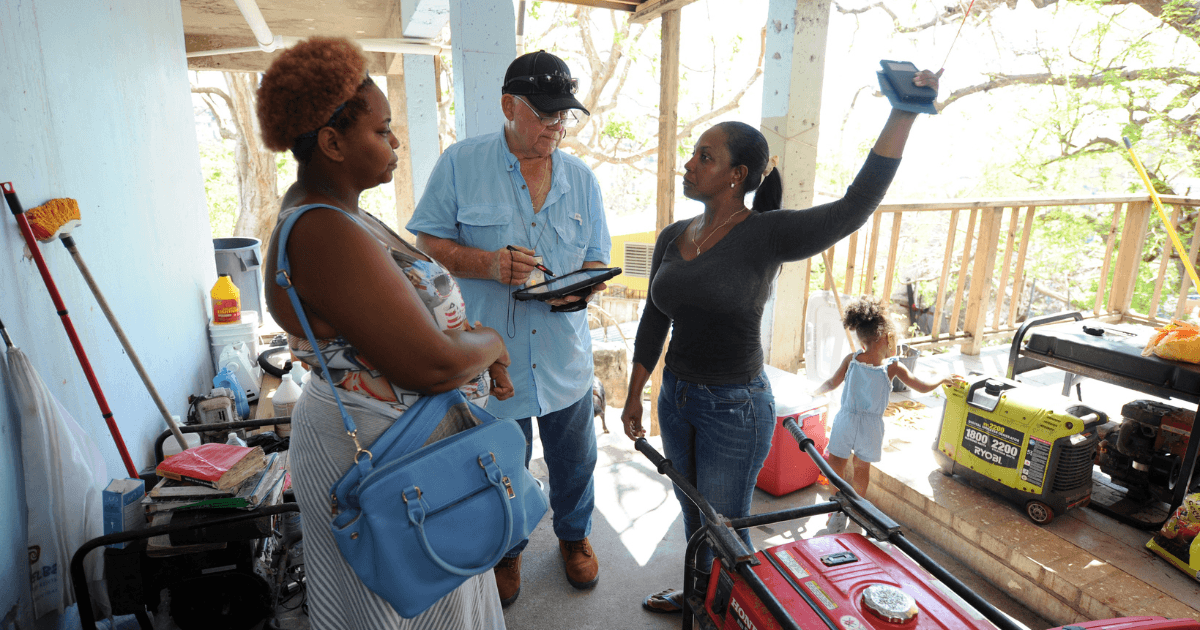
3) Response and Recovery Workers, also called disaster clean-up workers, are people who move into regions that have been affected by weather-related disasters to aid in clean-up and rebuilding. Entering a post-disaster area has significant associated health hazards, including risk of structural collapses; exposure to toxic substances including mold, pesticides, and asbestos; electrical shocks from downed power lines; carbon monoxide poisoning from unventilated generators; heat-related illnesses; and injuries related to heavy equipment. Worker training may be limited, and personal protective equipment may be unavailable. Availability of healthy food, clean water, and safe housing may also be limited.
Farmworker Health during Extreme Weather Disasters
When people move out of a service area, their health care often does not follow. Farmworkers who move regularly with the seasons, or who arrive in the US on an H-2A visa for a limited period, are frequently not connected with a medical home. They are also often the first and hardest hit in an extreme weather event. Farmworkers may be categorized as weather-impacted individuals. In some cases, however, they may be categorized as more than one type of displaced individual. For example, some farmworkers apply to become farmworkers in the US because weather disasters have reduced agricultural employment opportunities in their home country, but those same farmworkers may experience an extreme heat wave once they are working in the US. These farmworkers were weather-precipitated individuals before they became weather-impacted. After hurricanes Helene and Milton impacted farms across the south in 2024, farmworkers in North Carolina on H-2A visas received visa extensions to assist in cleanup of inundated fields. In this way, these weather-impacted individuals became response and recovery workers.
Farmworkers may be at higher risk of health implications from extreme weather because they:
- May be unfamiliar with the community, the local health center, and resources available to them in the case of a disaster;
- May have limited English proficiency, and weather alerts may not be translated;
- May live in extremely remote areas with few transportation options;
- May lack access to the internet and news sources, to learn about weather alerts and evacuation notices;
- May be reluctant to seek assistance or report dangerous working conditions for fear of jeopardizing their employment;
- Work outdoors with higher exposure to extreme weather;
- May have health-related factors that increase their risk, including:
- Pesticide exposure
- Dehydration
- Air pollution exposure
- Often work in areas like low-lying farms that may be at higher risk.
Other community members who are at higher risk of health complications during extreme weather include: children, those with low income, those with a preexisting chronic condition like diabetes, those who are pregnant, and older people.

Physical Conditions
Physical health conditions that may be impacted by a disaster include:
- Diabetes
- Heart disease
- Dementia
- Chronic obstructive pulmonary disease
- Asthma
In the example of diabetes, a farmworker who must rapidly leave their home needs to consider his treatment needs. Clinicians are encouraged to help patients with diabetes prepare for a disruption in care by considering:
Nutrition: Patients should be encouraged to prepare an emergency food container that contains diabetes-appropriate basics.
Treatment: Patients must be masterful when it comes to understanding diabetes, its impact on the body, and how the patient’s care plan stabilizes their blood sugars. When a disruption occurs, the patient who understands the signs and symptoms of hypo- and hyperglycemia will be able to take better care of themselves if monitoring systems fail or become unavailable.
Medication: Insulin must be kept cool. Discuss how to keep a low temperature when refrigeration is unavailable, like placing insulin in cool, clean water. Discuss what to do if medication gets warm; more insulin may not be available at the pharmacy if they had recently filled their prescription. Additionally, health centers must prepare to provide additional prescriptions after disasters.
Mental Health Impact
The emotional stress of a weather event affects everyone. Shock, emotional instability, stress reactions, and anxiety are some of the symptoms that may increase among patients who experience a disaster.
Some people may already experience a burden of mental health conditions before the disruption of a weather event. Some of the conditions that lead to poor mental health include: poverty and economic hardship; social isolation or limited social support; poor housing conditions including housing insecurity; lack of health insurance; few mental health services nearby; and limited access to workers’ compensation. Farmworkers often encounter one or more of these conditions.
Farmworkers also have unique vital conditions for a healthy life. For example, exposure to certain pesticides, particularly acute poisoning, is associated with a higher risk of depression. Some farmworkers have experienced situations like displacement, extreme weather, or other compounding events when relocating that can further increase their risk of mental health symptoms.
Practical Solutions to Prepare for Disaster-Related Disruptions of Care: Resources and Next Steps
Education
Community health centers can weave education and preventative measures into their disaster preparedness plans, so that patients and the community at large can prepare before an extreme weather event disrupts their care. A key resource is Migrant Clinicians Network’s (MCN’s) 87-page in-depth curriculum, “Building Capacity Among Community Health Centers to Address Weather-Related Extreme Phenomena on Agricultural Communities,” which was designed for Puerto Rico and US Virgin Islands health centers but is widely applicable to all clinicians and settings. The curriculum includes seven modules supplemented with dozens of resources in English and Spanish that clinicians can use with their patients.
For example, clinicians serving farmworker patients can provide education on prevention of risk at work. Proper chemical storage, including secure cabinets, chemical inventory, and use of personal protective equipment (PPE), reduces the risk of pesticide exposure during and after a disaster. The fourth module in the curriculum includes ideas and resources on issues like pesticides, non-point source pollution, safe water, heat-related illnesses, and more, to assist clinicians in preparing education for farmworker patients.
Continuity of Care Systems
A key element of an emergency plan is to determine pathways for patients to continue care if they must leave the service area during or after a disaster. Health Network is MCN’s longstanding care coordination program. Since 1995, Health Network has found care for over 15,000 patients who have moved across the United States and Puerto Rico. Health Network serves anyone with an ongoing health condition who must move before their treatment is completed.
Health care providers, community health workers, outreach workers, clinicians, and other community service professionals can enroll patients in Health Network through MCN’s online Health Network Portal or via fax, encrypted email, or phone. Once MCN receives complete enrollment information, Health Network will provide patient navigation and care coordination, finding patients a new health center and providing scheduling assistance, medical records transfer, follow-up support, and peer support. Health centers can encourage pre-enrollment as one aspect of emergency planning for highest-risk community members.
Pre-enrollment in Health Network ensures that the Health Network team has patient contact information, patient consent, and access to medical records, to rapidly assist patients in the case of a disaster. Clinicians can identify patients who have ongoing health needs who are most likely to have their treatment disrupted due to extreme weather. By pre-enrolling a patient, a clinician builds pathways to care that may be otherwise difficult to attain after a disaster. During or after a disaster, the clinician can notify Health Network that pre-enrolled patients will need assistance, and Health Network will begin its process to reach out to the patient and determine next steps for care.
- Learn more about Health Network: https://www.migrantclinician.org/healthnetwork
- Learn how to enroll: https://www.migrantclinician.org/enroll
Mental Health
Clinicians can access a wealth of mental health resources for their patients, including patients who are limited English proficient (LEP) or Spanish-speaking, on MCN’s Mental Health and Well-Being page: https://www.migrantclinician.org/mental-health-and-well-being
An example is the resource, “What is Self-Compassion and Why Is It Important?” which is available at: https://www.migrantclinician.org/resource/what-self-compassion-and-why-it-important.html
MCN’s newest comic book is “My Health Is My Treasure: Embracing Life with Diabetes.” Released in March 2026, this comic book offers simple, practical tools for managing stress and caring for well-being in everyday life for people who are living with diabetes while contending with other stressors like extreme weather.
Clinicians must also care for themselves in the event of a disaster, so they can continue to care for their communities. MCN’s Witness to Witness (W2W) serves those in high stress jobs who work with clients who are themselves experiencing high levels of stress. Dozens of resources in English and Spanish are available on the W2W webpage: https://www.migrantclinician.org/w2w
An example is the resource, “Helping the Helpers,” a comic book in English and Spanish on self-care for health care providers, available at: https://www.migrantclinician.org/resource/helping-helpers-comic-book.html
Other Resources: Visit MCN’s Webinars & Online Trainings page to view upcoming and recently archived webinars or sign up to receive alerts on upcoming trainings: https://www.migrantclinician.org/education-and-training